Memory fails
under pressure.
The record shouldn't.
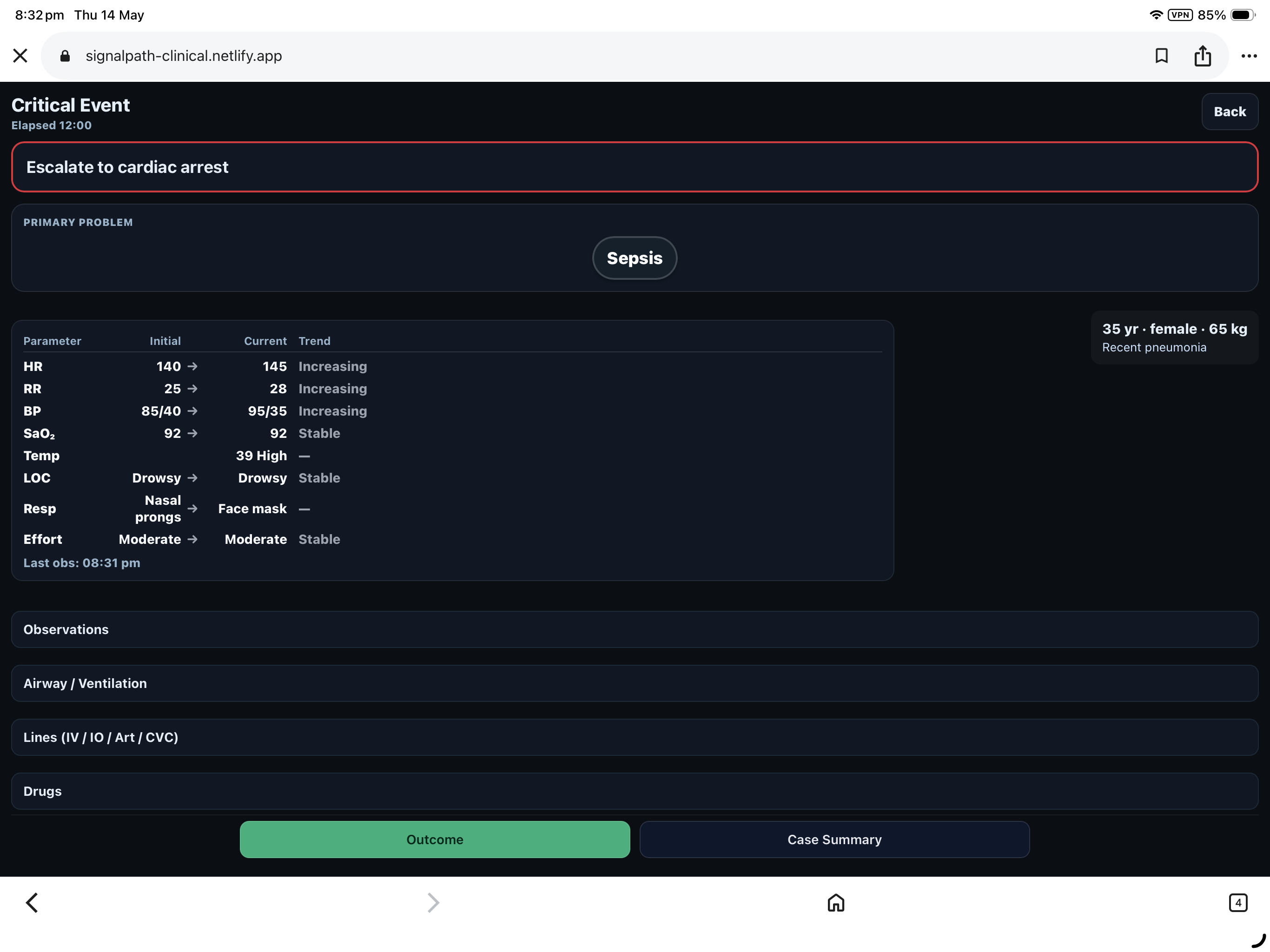
Real-time chronology for cardiac arrests, MET calls, retrievals, peri-intubation, and ICU escalation.
Four hours later, the most junior person in the room is asked to reconstruct what happened.
Their memory becomes the medical record.
The current standard isn't a standard.
It's damage control after the fact.
Scribbled notes. Fragmented chronology.
Paper notes, whiteboards, disconnected systems.
Drug times estimated.
Sequence reconstructed from recall.
Debrief without a sequence.
Written by the most junior in the room.
Coronial review asks what happened.
The answer is: we think.
Built for a tired, stressed, terrified junior at 3am.
Because that is who is holding the pager. Every interface decision was made for that person, at that hour, at that level of cognitive load.
Hand tremor. Gloved hands.
No precision input available during resuscitation. Targets sized accordingly.
Working memory failure under cortisol.
The scribe cannot also be a UI navigator. Each screen carries one decision.
Visual search costs seconds.
Information arranged by urgency. The most important value is the most visible.
If it works for them, it works for everyone.
Designed the way safety-critical systems are designed.
SignalPath draws on human-factors principles from disciplines where interface failures cost lives.
Aviation cockpit design
Information hierarchy under cognitive overload. Critical values always visible. Status before detail. Glance-readable at 200ms.
Black-box flight recorders
Every event timestamped as it occurs. Sequence preserved. Record immutable. Reconstruction possible at any later point.
Documentation infrastructure
The product records. It does not fly the plane. Clinical decisions belong to clinicians. SignalPath captures what was decided, when, and by whom.
CONFIGURATIONS
Cardiac arrests · MET calls · Retrievals · Peri-intubation · ICU escalation · Trauma resuscitation
After the event.
A structured, timestamped clinical event document. Generated locally. Controlled by the clinician.
The event is over in thirty minutes.
The record lasts as long as it needs to.
Provenance matters. So we'll say it plainly.
Built by a senior clinician. Not a technology company.
SignalPath was built by a senior clinician after years running cardiac arrests, MET calls, retrievals, and ICU emergencies. The product exists because the documentation problem is real, the people writing the record at 3am are exhausted, and the current tools are not enough.
Get SignalPath→ORIGIN
Australian-designed.
Internationally deployable.
For hospitals, retrieval services, expedition medicine, and any environment where critical events happen.
Direct contact
admin@signalpath.com.auGet SignalPath.
Available for iPad · iPhone · Android tablet. Clinician access required.